Bowel obstruction, also known as intestinal obstruction, is a mechanical or functional obstruction of the intestines which prevents the normal movement of the products of digestion. Either the small bowel or large bowel may be affected
Symptoms
4 Cardinal Signs of IO:
- Abdominal Pain
- Vomiting
- Abdominal distention
- Constipation
Other hx:
– Symptoms of GIT bleed, infection,
– Previous surgeries,
– Underlying GIT disorders,
– Risk factors for ischaemic bowel: atherosclerotic RH, heart disease, previous stroke
– Suspicion of malignancy: LOW, LOA, Previous Cancer, Family history of cancer
Physical Examination
Vitals: Is patient stable? Any fever? (sepsis) Hypotension, tachycardia? (dehydration)
General inspection: Abdominal distension? Cachexia? Confusion?
Peripheries: Look for signs of dehydration e.g. capillary refill, dry tongue, palpate lymph
nodes
Per Abdomen
– Any distension?
– Scars from previous abdominal surgery?
– Visible peristalsis? – severe obstruction
– Signs of peritonitis: guarding, rebound tenderness, or SNT
– Masses, hernia – inguinal + femoral (more likely strangulated)
– Bowel sounds (Initially hyperactive, later may be sluggish or absent)
Per Rectal: any masses felt, any impacted stools?
Investigations
| FBC | Anemia, raised WCC |
| RP | Dehydration due to (or acute renal failure from dehydration) – Intraluminal 3rd Space Loss (damaged enterocytes unable to reabsorb) – Vomiting (also assess K+ loss: can perpetuate paralytic ileus) |
| ABG | – Acidosis from bowel ischemia – Alkalosis due to vomiting (more for pyloric stenosis in children) – Lactate (ischemic bowel) |
| Amylase | acute pancreatitis (AXR may just show small bowel dilatation) |
| AXR | bowel dilatation fecal loaded |
Management
1. Rehydration/ resus + correct electrolyte imbalance
- use NS + KCL (even electrolyte normal as we anticipate E/I)
- how much? – based on pt’s weight & requirement
2. Keep NBM – 70% recover with bowel rest and decompression
3. NG tube suction
– Large bore NG tube (small diameter easy to get blocked up)
– Either passive connection or low-intermittent suction
Passive – tubes placed on free drainage with 4-hourly aspiration
Continuous / intermittent – suck intermittently till bowel wall collapse, useful
for patients with estimated high NG tube o/p
2. HCO3 if indicated
3. Antibiotic
- as there’s risk of bacteria translocation
- if suspect ischemic bowel, bowel perforation
- IV Cefobid 1g BD and IV Flagyl 500mg TDS
5. Monitoring
- VS
- I/O chart – insert CBD, CVP
- biochemical
Conservative management – within 48-72 hours..
Differential Diagnosis (DDx)
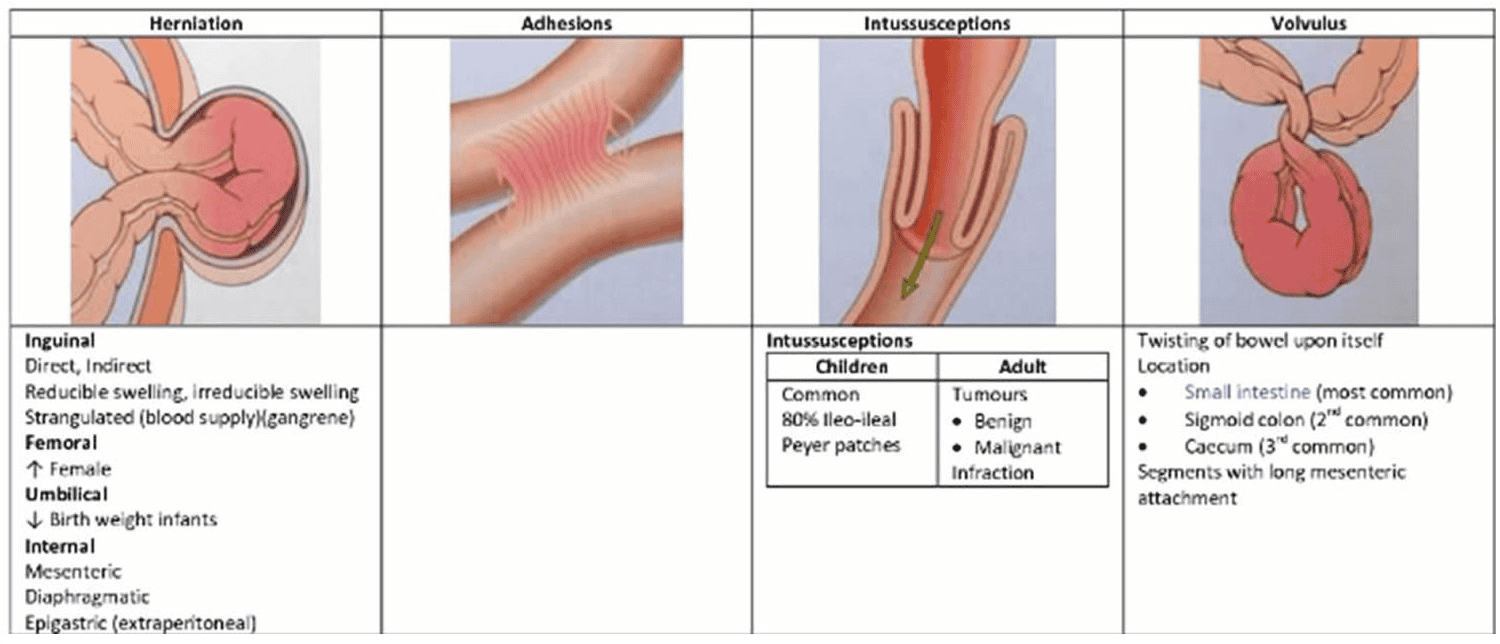
Intestinal obstruction secondary to :
- Abdominal adhesions. These are growths of tissue in bands that may force your intestines out of place.
- Hernia. A hernia is a split in the muscle wall of your abdomen. Hernias can cause bulges and pockets. These may block your intestine.
- Volvulus. A volvulus happens when part of your intestine twists around itself. This creates a blockage.
- Intussusception. This condition means that a segment of your intestine slides into another segment. This narrows but may not block your intestine.
- Scarring. When your body heals small cuts (wounds), scar tissue forms. This can happen inside your intestine as well. These scars can build up and create partial or total intestinal blockages. Scarring can result from tears in your intestinal wall, belly (abdominal) or pelvic surgery, or infections.
- Inflammatory bowel disease. Crohn’s disease and ulcerative colitis are 2 examples.
- Diverticulitis. Tiny pouches (diverticulae) can grow off the large intestine lining. These may become inflamed.
- Tumors. Growths may be cancer or harmless (benign). Either way, they can block your intestine completely or partially.
- Foreign objects. Nonfood objects that you swallow on purpose or accidentally may cause partial or complete intestinal obstruction.
- Meckel diverticulum. About 2 in 100 people are born with this additional small pouch inside the intestine.
Prevention
Basically, the possibility of preventing intestinal obstruction and adhesions depends on the causative agent. In fact, some cases of intestinal obstruction can not be prevented in any way. However, you can reduce the risk of intestinal obstruction by doing the following:
- Treat hernias and similar injuries as soon as possible before the bowel obstructs.
- Reduce the risk of stool compression and diverticulosis (wall protrusion) of the colon through:
* Eat plenty of fiber-rich foods
* Drink plenty of water and fluids
* Exercise regularly




